
Abstinence Education Links
SPIRITUAL PREPARATION
- Adoration: Prepare your presentation in the presence of the Blessed Sacrament. Go over your talk with God, and He will place new inspirations on your heart. Spend time in adoration before (and after) the presentation. To find an adoration chapel near you, click here. Mother Teresa often prayed the Fragrance Prayer and her Prayer Before Leaving for the Apostolate. Do the same.
- Mass: Before your presentation, try to attend a morning Mass. To find Mass times near where you’re speaking, click here. Offer up the Mass for your audience and their families. In the words of St. John Chrysostom, “The Eucharist is a fire that inflames us, that, like lions breathing fire, we may retire from the altar being made terrible to the devil.”
- Confession. If possible, receive the sacrament of reconciliation at some point in the days preceding your presentation.
- Entrustment. Consecrate your presentation to Our Lady. Mother Teresa often prayed what she called the express novena. She knew that it was so powerful that she would pray it—not so much in petition for something—but in thanksgiving for the fact that she knew she was going to obtain it. It consisted of praying the Memorare nine times in a row. Memorize this prayer and pray it before each talk in thanksgiving for the conversions that will take place.
- Guardian Angels. In 2 Kings 6, a great battle is described. In the midst of it, a servant approached the prophet Elisha, crying out in despair that their troops were vastly outnumbered. Elisha knew that God would deliver them and he was aware of a spiritual presence that the servant wasn’t. He said, “Fear not, for those who are with us are more than those who are with them.” He then prayed, “O Lord, I pray thee, open his eyes that he may see.” Before the servant’s eyes, he suddenly beheld the mountain filled with fiery horses and chariots around Elisha. The angelic warriors led them to complete victory. Everyone has a guardian angel, but we rarely call to mind their constant presence or invoke their powerful intercession. Before your presentation, pray to your guardian angel. You could ask him to lead a Rosary with all of the guardian angels of every student and teacher present in the auditorium throughout the duration of your talk. Even if a student is an atheist, he still has a guardian angel. Therefore, it is wise to take advantage of this heavenly host. As Christians, we must never overlook this legion at our side.
- Holy Spirit. Pray to the Holy Spirit for the gift of apostolic preaching. Ask for the eloquence of speech of St. Anthony of Padua, the effectiveness of speech of Samuel, and for gifts even greater than these to touch the hardest of hearts.
- Fast. Do not forget to fast for your audience. If you are unfamiliar with the practice, consult a priest or spiritual director.
- Intercession. Ask others to pray for your presentation. Send out emails and tweets to let others know you need their prayers. See if a friend, family member, priest, or nun would be willing to be in Eucharistic Adoration during your talk. Some convents even have online forms where you can submit prayer petitions.
MENTAL PREPARATION
“Prepare your words and you will be listened to; draw upon your training, and then give your answer.” (Sirach 33:4)
Read good books, such as:
- Soul of the Apostolate, by Jean-Baptiste Chautard
- Love and Responsibility, by Pope John Paul II
- The Way, by St. Josemaria Escriva
- Good News About Sex and Marriage, by Christopher West
- If You Really Loved Me, by Jason Evert
Research: Familiarize yourself with research on STDs, birth control, and other important statistics such as sexual activity rates.
LOGISTICS
Besides spiritual and intellectual preparation, here are some practical tips to help your presentation go smoothly.
DELIVERY
Click here for tips on how to deliver a powerful presentation.
MEDIA
If you have an opportunity to speak with the media, here are a few tips for handling them instead of letting them handle you:
- Smile. Loosen up, and don’t get defensive.
- Be exciting. People who work on television or radio use exaggerated expressions and voice inflections. When you watch them from home or listen in the car, you hardly notice it. Then, watch or hear an interview with a person who isn’t accustomed to being in front of the camera or on radio. Because they speak in a normal way, they sound boring and half-asleep. Just as the voice is important in radio, the image is important on television. In a presidential debate between John F. Kennedy and Richard Nixon, those who listened to the debate overwhelmingly thought that Nixon won, while those who watched the debate and were able to look at the candidates thought that Kennedy won. He appeared more at ease, and even though his mere words may not have been as convincing as those of Nixon, his presence and composure were enough to make up for it. One way to grasp the importance of one’s image is to ask yourself who would win a debate if there was no sound.
- Know your talking points. Before an interview, think of the three or four positive points that you want to get across. If you are in a debate or getting interviewed by someone who is unfriendly to the message of chastity, don’t get controlled, but know your agenda. As they say, “Answer the question you wish you had been asked.”
- Be Humble. If you get stumped by a question, follow the wisdom of Sirach 6:13-14, “Be swift to hear, but slow to answer. If you have the knowledge, answer your neighbor; if not, put your hand over your mouth.”
- Be Yourself. Don’t try to emulate someone else’s style. Authenticity is key.

Want to become a chastity speaker? Here are seven steps to get started:
1. Pray.
If you are willing to speak to a million people, are you willing to pray and fast for as many? You don’t need a stadium to reach the masses. You just need to offer your Masses. Your zeal for souls is a great thing. Therefore, entrust your desires to God, and ask that the doors would open in His time.
2. Read Soul of the Apostolate.
This classic, by Jean-Baptiste Chautard, will help you understand the importance of step one.
3. Continue your education.
If you’re not yet in college, choose a solid Catholic college, if possible. In the meantime, read great books, such as Love and Responsibility by Pope John Paul II, or a simplified version of it, such as Men, Women, and the Mystery of Love, by Dr. Ted Sri. To teach chastity, you don’t need a degree in Theology, although it helps. To further your education without having to get a four-year degree, look into the immersion courses offered at the Theology of the Body Institute. These are brief, intense courses offered to deepen your grasp of the Church’s teaching on human sexuality through the lens of the Theology of the Body.
4. Bloom where you’re planted.
Instead of strategizing ways to speak internationally, find ways to promote purity in your own community. Here are several ways to begin:
-
Contact local Crisis Pregnancy Centers to see if they run an abstinence program, and ask if they need any help. Many of them do work in schools and churches in your community to promote abstinence.
-
Volunteer for a local youth group. Through retreats and teaching nights, you should have plenty of opportunities to witness to others about chastity. Life Teen is a great place to begin.
-
If you know a religion teacher at a local Catholic high school, ask if you and some friends can speak about chastity in a classroom to the students.
-
Start a chastity club on your high school or college campus.
-
Launch a chastity project.
-
Your diocese may have a chastity program, and may be looking for volunteers. By calling the diocesan offices in your area, you may find an opportunity. In particular, ask for the diocesan directors of youth ministry, pro-life, and marriage and family.
-
Contact the National Abstinence Clearinghouse. They may be able to point you to abstinence movements that are looking for volunteers in your area. Also, contact them at info@abstinence.net and get on thier email list, so you’ll stay up to date on the latest news and developments in abstinence education, STDs, legistlation, etc.
5. Serve.
Once you’ve spent some time ministering in your own area, consider serving on a missionary team. Here are four great apostolates to consider:
-
The Culture Project
-
NET Ministries
-
FOCUS (Fellowship of Catholic University Students)
-
Generation Life
-
Missionaries of Purity
6. Plan wisely.
If you’re looking for full-time employment as a chastity speaker, realize that speakers typically never start as speakers. Most of them first held jobs as youth ministers, diocesan directors of youth ministry, high school teachers, and such. It takes at least five years of public speaking before people will know of you, and during this ramp-up time, you would not be able to support yourself unless you had another profession to financially sustain you. This other profession doesn’t need to be a religious one. You could pursue any career, while teaching chastity on the side, thorough any of the volunteer opportunities mentioned above.
7. Prepare your talk.
Click here for tips on how to give a chastity talk.
It might help to know that your friend is not on a quest for sex. Perhaps your friend has some hurt or loneliness in her life, and she figures that if she has sex, it will feel like love and security, and she will be happy. Or perhaps she’s just curious and too immature to realize the consequences of sex. Either way, if you look into her heart you will see that she is not longing for a series of physical relationships with random guys. She is looking for enduring love and for intimacy, to be accepted by a man and cared for by him.
Your friend deserves these things, but she needs to be careful and courageous so that she does not fall for a counterfeit. There are plenty of boys out there who will tell her how beautiful her eyes are and how much they love her and will “always” be there. They will give her “love” for the sake of getting sex, and she may want to give them sex for the sake of feeling loved. Her heart is made for something better than this, and so she needs to realize that she is worth the wait. She cannot find happiness otherwise. As the Bible says, “She who is self-indulgent is dead even while she lives” (1 Tim. 5:6).
The following are some of the bad effects of premarital sex; do not dwell on them any longer than is necessary to give her a reality check. What she needs more than the bad news about premarital sex is the good news about what she is worth and what plans God has in store for her. She needs to be encouraged to wait not because sex is bad but because real love is so good.
The negative consequences of premarital sex can be seen from the relational, physical, emotional, and spiritual points of view.
Relationships:
Consider how premarital sex can affect relationships. One high school girl wrote, “I am sixteen and have already lost my virginity. I truly regret that my first time was with a guy that I didn’t care that much about. Since that first night he expects sex on every date. When I don’t feel like it, we end up in an argument. I don’t think this guy is in love with me, and I know deep down that I am not in love with him either. This makes me feel cheap. I realize now that this is a very big step in a girl’s life. After you have done it, things are never the same. It changes everything.”[1]
Another young person said, “I slept with many, many people trying to find love, to find self-worth. And the more people I slept with, the less self-worth I had.”[2] Some people may argue, “Well, what if I really care about him or her? I think sex will bring us closer together.” Indeed, sex creates a bond. However, 80 percent of the time, the physical intimacy of a teen’s first sexual relationship won’t last more than six months.[3] Couples who want what is best for their relationship or future marriage will have the patience to wait.
Most of the time, when a girl gives away her virginity, she assumes the relationship will last forever. However, click here and scroll down to page 4 of the document, under the first graph. Look at your friend’s age at the bottom, and it will tell you how many more sexual partners she will probably have if she plans on losing her virginity now. If she’s like most freshmen, she’s probably 14 years old. This study of more than 10,000 women shows that when a girl loses her virginity at that age, she’ll probably have about thirteen more lifetime sexual partners.
Beyond one’s relationship, premarital sex frequently causes tension within families because of the dishonesty that usually accompanies the hidden intimacies. Relationships with friends are often strained, and when things turn sour, the gossip and social problems often become unbearable. Everyone talks about how hard it is to say no to sex, but no one tells you how hard it is when you say yes.
Physical:
In regard to the physiological side of things, it is dangerous for a young single woman to be sexually active. Because a teenage girl’s reproductive system is still immature, she is very susceptible to sexually transmitted diseases (STDs).[4] (Click here for the biological explanation.) In fact, early sexual activity is the number one risk factor for cervical cancer, and the second is multiple sexual partners.[5] A girl’s body, like her heart, is not designed to handle multiple sexual partners.
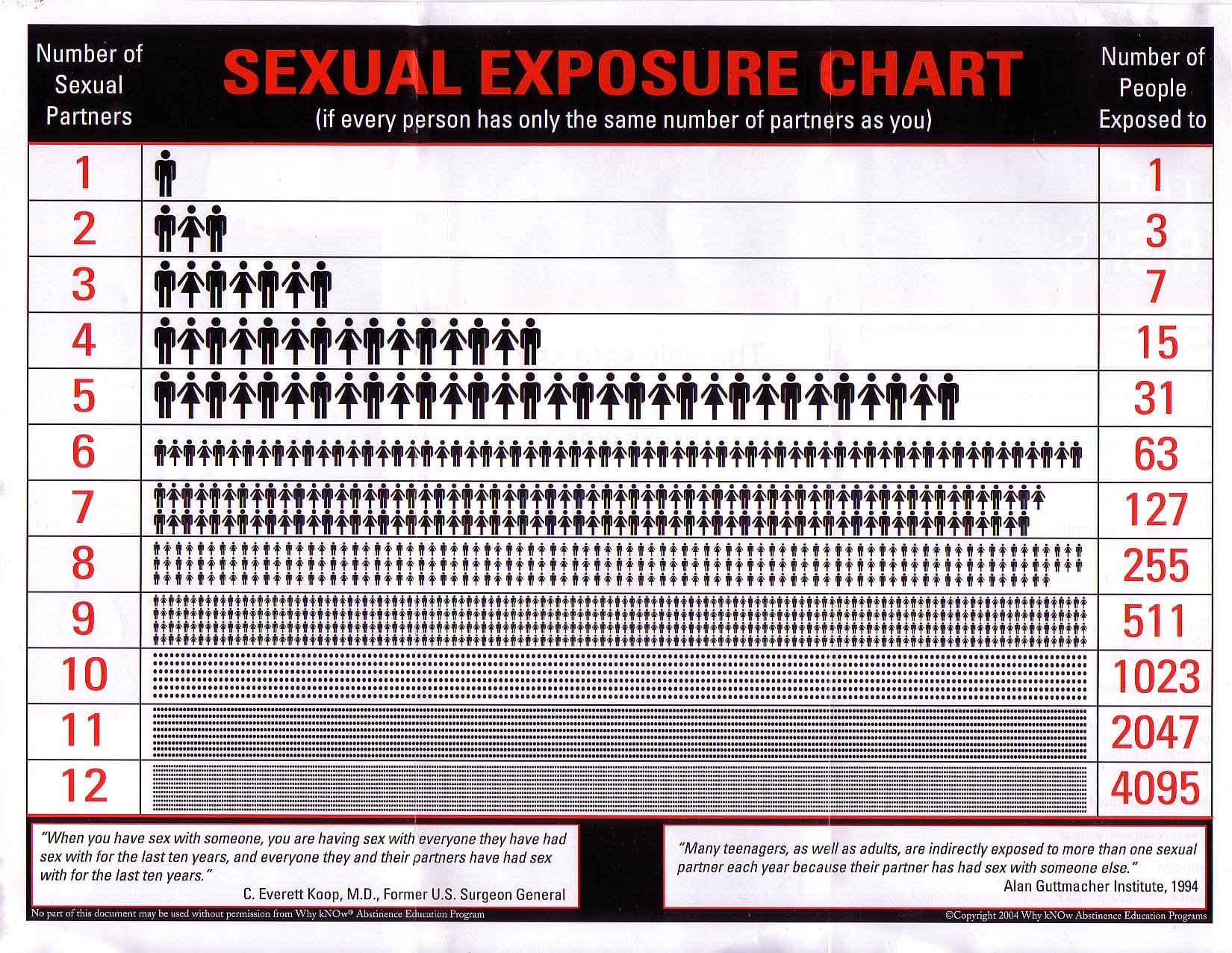
While your friend might plan on sleeping with only one guy, she could be exposing herself to the STDs of hundreds of people through a single act of intercourse. Here’s how: Scientists studied the sexual activity of a public high school of about one thousand students.[6] About half (573) of the students had been sexually active, and most of them had only been with one partner. However, when the scientists tracked the web of sexual activity among the students, it was discovered that more than half of the sexually active teens—without knowing it—were linked together in a network of 288 partners within the school! (Click here to see the web of this sexual activity.) So if your friend slept with a guy from this school, theoretically she could be in bed with one-fourth of the entire student body.
Emotional:
The emotional side effects of premarital sex are also damaging to a young woman. One of the most common consequences of teenage sexual activity is depression. Girls who are sexually active are more than three times as likely to be depressed as girls who are abstinent.[7] In fact, the condition has become so predictable that the American Journal of Preventive Medicine recommends to doctors: “[Girls who are engaging in] sexual intercourse should be screened for depression, and provided with anticipatory guidance about the mental health risks of these behaviors.”[8] Even if a girl experiments with sex once, research shows an increased risk of depression.[9] Also, consider the fact that the rate of suicide attempts for sexually active girls (aged twelve to sixteen) is six times higher than the rate for virgins.[10] Tragically, these girls do not realize the purity, hope, and forgiveness that they can find in Christ.
Unfortunately, many young women search for meaning only in relationships with guys, instead of with God. It is not uncommon for a girl to have sex in order to make a guy like her more or to encourage him to stay with her. She may compromise her standards because she is afraid of never being loved. Once he leaves her, though, an emotional divorce takes place. A person’s heart is not made to be that close to a person and then separated.
Since teenage sexual relationships rarely last, the girl’s sense of self-worth is often damaged. She may conclude that if she looked better, he would have stayed longer. This mentality can lead to harmful practices, such as eating disorders. Or the disappointment she feels may drive her into a state of self-hatred. Some young women even begin to hurt their own bodies in an attempt to numb the emotional pain. Such practices never solve the problems, though. If she wants to be loved, she needs to begin by loving herself.
In her heart, a girl who has been used knows it. However, she may immediately jump into another sexual relationship to escape the hurt. If she tries to boost her self-esteem by giving guys what they want, then her self-worth often ends up depending upon those kinds of relationships. Her development as a woman is stunted because without chastity she does not know how to express affection, appreciation, or attraction for a guy without implying something sexual. She may even conclude that a guy does not love her unless he makes sexual advances toward her. She knows that sex exists without intimacy, but she may forget that intimacy can exist without sex. A girl on this track usually feels accepted initially, but that acceptance lasts only as long as the physical pleasure.
Such a lifestyle will also take its toll on her ability to bond. Here’s why: Sharing the gift of sex is like putting a piece of tape on another person’s arm. The first bond is strong, and it hurts to remove it. Shift the tape to another person’s arm, and the bond will still work, but it will be easier to remove. Each time this is done, part of each person remains with the tape. Soon it is easy to remove because the residue from the various arms interferes with the tape’s ability to stick.
The same is true in relationships, because neurologists have discovered that previous sexual experiences can interfere with one’s ability to bond with future partners.[11] This does not mean that if a person is not a virgin on the wedding night, he or she will be unable to bond with a spouse. It simply means that when we follow God’s plan, we have the most abundant life possible. But when we turn from his designs and break his commandments, often we are the ones who feel broken afterward.
Spiritual:
Sin cuts us off from God, and this is the most serious consequence of premarital sex. After going too far, many of us know all too well the cloud of guilt that weighs on our hearts. The solution is not to kill our conscience but to follow it to freedom. It is calling us, not condemning us. Provided we repent, God will be there to welcome us home and let us start over (see John 8 and Luke 15).
What this all means is that our bodies, our hearts, our relationships, and our souls are not made for premarital sex. We are made for enduring love.
_______________________
[1]. Thomas Lickona, “Sex, Love, and Character: It’s Our Decision” (address given to assembly of students at Seton Catholic High School, Binghamton, N.Y., January 8, 1999), 10.
[2]. All About Cohabiting Before Marriage, “Myths About Cohabitation,” http://www.leaderu.com/critical/cohabitation-myths.html.
[3]. Suzanne Ryan, et al., “The First Time: Characteristics of Teens’ First Sexual Relationships,” Research Brief (Washington, D.C.: Child Trends, August 2003), 5.
[4]. A. B. Moscicki, et al., “Differences in Biologic Maturation, Sexual Behavior, and Sexually Transmitted Disease Between Adolescents with and without Cervical Intraepithelial Neoplasia,” Journal of Pediatrics 115:3 (September 1989), 487–493; M. L. Shew, et al., “Interval Between Menarche and First Sexual Intercourse, Related to Risk of Human Papillomavirus Infection,” Journal of Pediatrics 125:4 (October 1994), 661–666.
[5]. R.A. Hatcher, et al., Contraceptive Technology (1994), 515. [6]. Peter Bearman, et al., “Chains of Affection,” American Journal of Sociology 110:1 (July 2004), 44–91.
[7]. Robert E. Rector, et al., “Sexually Active Teenagers are More Likely to be Depressed and to Attempt Suicide,” The Heritage Foundation (June 3, 2003) .
[8]. Hallfors, et al., “Which Comes First in Adolescence—Sex and Drugs or Depression?” American Journal of Preventive Medicine 29:3 (October 2005), 169.
[9]. Hallfors, et al., 168; Hallfors, et al., “Adolescent Depression and Suicide Risk: Association with Sex and Drug Behavior,” American Journal of Preventive Medicine 27:3 (October 2004), 224–231; Martha W. Waller, et al., “Gender Differences in Associations Between Depressive Symptoms and Patterns of Substance Use and Risky Sexual Behavior among a Nationally Representative Sample of U.S. Adolescents,” Archives of Women’s Mental Health 9:3 (May 2006), 139–150.
[10]. As reported by D. P. Orr, M. Beiter, G. Ingersoll, “Premature Sexual Activity as an Indicator of Psychological Risk,” Pediatrics 87 (February 1991), 141–147.
[11]. Joe McIlhaney and Freda McKissic Bush, Hooked (Chicago: Northfield Publishing, 2008).
The easiest way to know if you are ready to have sex is to look at your left hand. If you do not see a wedding ring, you are not ready for sex. This may seem like a simplistic answer, but look at the logic behind it. What does it mean to be ready for sex?
Sex cannot be reduced to a biological act. Every aspect of the person is affected: the body, heart, mind, soul . . . and your future. Therefore, a person is physically able to have sex long before he or she is ready for its consequences. But instead of zeroing in on the negative consequences, it is more important for a person to understand the meaning of sex. Then it becomes clear when we are “ready” for it.
We are commonly told with regard to sex, “Just say no.” Why? “Because sex before marriage is bad.” But what kind of answer is that? Most people have never been told why—why sex within marriage is so good and beautiful and why sex outside of marriage is a counterfeit of the love that we have been created to give and receive. Instead of fear tactics, we need to hear the truth about the goodness and beauty of sex and God’s plan for love.
To help us understand the gift of our sexuality, Pope John Paul II gave the Church a series of teachings known as the “Theology of the Body.” In it he explained that when we accept the demands of love and live according to the truth of our sexuality, we make visible in our bodies the invisible reality of God—that he is love. If we don’t understand this deeper meaning of sex, marriage may seem like nothing more than a piece of paper that legalizes intercourse. Once we are aware of the greatness of the gift of sex, we will have an attitude of reverence toward it, and only with God’s permission will we lift the veil of its mystery. This demands faithfulness to him while we are waiting to find our spouse. And we can start preparing for a good marriage right now by avoiding anything that could harm a relationship with a future spouse.
If a person does not understand the meaning of sex, he or she may give it away to the first bidder. Some say that they want to save the gift of sex for the “right” person, someone they really love. But strong feelings of love do not make a person ready for sex. This is clear in sexually active couples who are afraid of what sex means. They fear that their lovemaking could bring forth life. They also hide what they are doing from those who love them, such as their parents, and they fear that the incredible bond they have created might not be permanent.
Within marriage no such fears exist. Instead a husband and wife are ready to give and receive each other without reservation. They understand that sex is like saying wedding vows with your body. It is making a complete gift of yourself to another person.
When a person understands the meaning of sex, it becomes obvious that premarital sex is dishonest: it is a lie in the language of the body. With your body you are saying, “I give myself to you entirely. There is nothing more of me that I could give you,” but in reality there is no such commitment and gift of self. There is a total physical gift but no total gift of the person. The gift is reduced to a loan or a lease, because the body is given to the other temporarily. In other words, you are ready to have sex when your body speaks the truth: “I am entirely yours. Forever.” Therefore, only in marriage can one be “ready” for sex.
To read about some of the consequences of sexual activity before marriage, click here.
Billions of condoms have been shipped to Africa in order to prevent the spread of HIV.[1] However, countries that have relied on such “protection” to curb the epidemic are not seeing any great decline in the virus.[2]
One nation that clearly demonstrates this problem is Botswana. For over a decade Botswana has relied upon widespread availability of condoms in order to combat AIDS. Campaigns for abstinence and fidelity were not emphasized. Instead, billboards about “safe sex” lined the streets, while schoolchildren learned songs about condoms. According to The Washington Post, “The anti-AIDS partnership between the Bill & Melinda Gates Foundation and drugmaker Merck budgeted $13.5 million for condom promotion—25 times the amount dedicated to curbing dangerous sexual behavior. But soaring rates of condom use have not brought down high HIV rates. Instead, they rose together, until both were among the highest in Africa.”[3]
Unfortunately, Botswana was not the only nation to make this mistake. The journal Studies in Family Planning pointed this out in their article “Condom Promotion for AIDS Prevention in the Developing World: Is It Working?” Its authors noted that “in many sub-Saharan African countries, high HIV transmission rates have continued despite high rates of condom use. . . . No clear examples have emerged yet of a country that has turned back a generalized epidemic primarily by means of condom promotion.”[4]
However, there is a clear example of an African nation turning back the epidemic of AIDS by other means. In the late 1980s Uganda was viewed as the worst nation in the world in terms of HIV/AIDS infections.[5] In 1991, 22 percent of people in the country were infected with HIV. By 1999 the number had dropped to 6 percent.[6] Ugandan President Yoweri Museveni insists that their unique success among African countries is due to their behavioral approach. He said, “In comparison with other countries per capita expenditure on condoms, we spend far below other developed countries, which emphasize use of condoms in their fight against the disease.”[7] Instead of placing the primary emphasis on condoms, they emphasized abstinence and faithfulness first. As a result, they have experienced the greatest decline in HIV in the world.[8] According to the Journal of International Development, it was “the lack of condom promotion during the 1980s and early 1990s [that] contributed to the relative success of behavior change strategies in Uganda.”[9]
Some “safer sex” advocates attempted to claim credit for the success of Uganda’s AIDS decline. But Dr. Edward Green, a Harvard senior research scientist, ruled out such a connection, since “Uganda shows a significant decline in STDs in the absence of a male condom prevalence rate over 5 [percent].”[10] In fact, condoms were not widely used in Uganda until after much of the HIV decline had already taken place.[11] The real reason for the drop in HIV is that between 1989 and 1995 casual sex in Uganda declined by 65 percent.[12]
Some of the sharpest declines took place within the teenage population, which the experts said “took many of us by surprise, since we believed that teenagers are driven by ‘raging hormones,’ therefore abstinence is an unrealistic or impossible objective.”[13] In the words of Dr. Green, who has over two decades of experience in Africa and had previously advocated widespread condom distribution, “Weren’t ‘we’ supposed to teach ‘them’ how to prevent AIDS?”[14]
Unfortunately, the success in Uganda has been undermined in recent years. According to The Washington Post, “The Ugandan turnaround was well underway by the time foreign AIDS experts began to arrive in the early 1990s, bringing with them the Western public health approaches—and values. They began to retool Uganda’s AIDS prevention efforts away from abstinence and fidelity—goals that many Westerners felt were unrealistic. As condom use increased, the percentage of young singles having sex rose from 27 percent to 37 percent between 1995 and 2000.”[15] It seems that only sex-saturated Westerners (who have no handle on their own STD epidemics) are naive enough to expect that condoms will solve the AIDS problem.
Some people ridicule the idea that abstinence education is a realistic way to deal with the AIDS crisis in developing nations. However, the evidence in favor of such an approach is becoming increasingly difficult to ignore.[16] In his testimony before the U.S. House of Representatives, Dr. Green said, “Many of us in the AIDS and public health communities didn’t believe that abstinence or delay, and faithfulness, were realistic goals. It now seems we were wrong.”[17]
In a Washington Post article entitled “Let Africans Decide How to Fight AIDS,” he added, “Billions of dollars and the lives of countless men, women, and children will be wasted if ideology trumps proven health policy.”[18] Lest anyone think that such an emphasis on abstinence is the result of conservative religious leaders placing their ideologies above science, Green noted, “I’m a flaming liberal, don’t go to church, never voted for a Republican in my life.”[19]
His appreciation for the effectiveness of promoting abstinence comes from witnessing its results. Had South Africa implemented Uganda’s emphasis on self-control, one scientist noted, “3.2 million lives would be saved between 2000 and 2010.”[20] The effectiveness of the Ugandan approach has led scientists to consider it a “social vaccine” against HIV.[21]
Why has the behavioral approach of reducing sexual partners been so much more effective than condom distribution? There are a number of reasons.
One reason is that most people do not use the condom consistently and correctly, even after being given sex education. In one study of over five hundred couples who were repeatedly advised by their clinicians to use condoms, only 8 percent of them used it consistently, despite the fact that they knew one partner had herpes and the other did not![22] In studies of relationships where one partner was infected with HIV and the other was not, only about 50 percent of them always used a condom![23] If those couples were not motivated enough to use the condom consistently, it’s hard to imagine that perfect condom use will ever be seen in the general population.
Some might assume, “Well, at least some protection is better than none.” This would seem to be a logical argument. After all, condom use can reduce the odds of HIV transmission during an act of intercourse. However, one study of over seventeen thousand people in Africa showed that inconsistent condom use was not protective against HIV.[24] In the presence of an epidemic, unless a person changes his or her behavior, it may be only a matter of time before he or she is infected. For this reason Dr. Norman Hearst said that he feared that we are “raising a generation of young people in Africa that believe that condoms will prevent HIV.”[25] While condoms may reduce the risk of HIV transmission, they do not “protect” against AIDS. When people are not taught the difference and are left thinking that risk reduction equals protection, they are more open to taking risks that they cannot afford.
A second reason why the “safe sex” message has failed to curb AIDS is that the “protection” offered by the condom decreases with repeated exposures.[26] A study funded by the Centers for Disease Control followed sexually active young women (most of whom had a steady boyfriend) to assess condom effectiveness over time.[27] The study found that those who used condoms consistently and correctly were not statistically less likely to acquire at least one STD than the girls who used condoms inconsistently or not at all. According to Dr. J. Thomas Fitch, “This study illustrates what happens over time with numerous acts of sex with an infected partner even when a condom is used.”[28]
Similar observations have been seen in Africa. Edward Green remarked, “Twenty years into the pandemic there is no evidence that more condoms leads to less AIDS. . . . Over a lifetime, it is the number of sexual partners [that matter]. Condom levels are found to be non-determining of HIV infection levels.”[29]
A third reason why condoms have failed to stop AIDS is that when a person is infected with other STDs, they are up to five times as likely to get HIV if exposed. There are several reasons why this occurs.[30] One reason is that many STDs cause sores that can serve as portals of entry for the virus. For example, a woman’s reproductive tract is often able to protect her from HIV.[31] However, this natural barrier is compromised when she is infected with certain STDs.[32] Considering that the number one determinant of STD infection is multiple sexual partners, any strategy to stop HIV that does not reduce sexual activity will have limited effect. This is why one AIDS researcher remarked that safe sex “has not been safe in the UK, and in Africa it has been positively dangerous.”[33]
One final reason why condoms have not stopped HIV is that those who are promiscuous more easily catch the virus. In fact, there would be a massive decline in the sexual transmission of HIV if people practiced six months of abstinence between sexual partners. This statement might sound absurd to anyone unfamiliar with the infectivity rates of HIV. The infectivity rate of a disease or virus measures the likelihood of its transmission. For HIV it is estimated to be .001, meaning that, on average, the odds of being infected with HIV through a single act of intercourse (without a condom) is about one in a thousand.[34] However, when a person is first infected with HIV, he or she is highly contagious.[35] If this person were to get tested for HIV right away, the test would show that he or she is HIV negative, despite the fact that he or she does have the virus and can easily transmit it!
Here’s why: Technically the HIV test does not look for HIV, but for antibodies against the virus. Antibodies are what your body produces to fight off intruders. But viruses are smart and they are often able to avoid being detected. HIV can hide in your body for months before your immune system recognizes it (and years before you know of it). So if your body does not know that you have been infected with HIV, it won’t produce antibodies to attack the virus. According to Dr. Harvey Elder, a professor of HIV/AIDS Epidemiology and Care, “The patient’s ‘HIV’ test becomes positive 4–24 weeks after exposure.”[36] But if the HIV test doesn’t find the antibodies, the doctors will tell you that you’re HIV negative.
Meanwhile, inside the body of a newly infected person, the HIV plasma viral level is very high, especially in the genital fluids (semen and cervical-vaginal fluids), because antibodies haven’t been produced to reduce their levels. Since the viral load is extremely high, and the person is shedding viruses, the infectivity rate soars in the early weeks of infection. Dr. Harvey continued, “During the first few months, a person infects 20–30 percent of sexual contacts but [the] HIV test is negative. When the test is positive, 0.2–0.3 percent of sexual contacts become infected [if there are no other STDs present].” This means that if people abstained from sex at least six months between partners, the odds of HIV transmission would be decimated. Therefore, countries that encourage monogamy and self control enjoy much greater success in preventing HIV than countries that simply hand out condoms.
A key example of this is in the Philippines, where condoms are rare, and so is HIV. A New York Times article entitled “Low Rate of AIDS Virus in Philippines Is a Puzzle” reported that the Church in the Philippines is “conservative and politically powerful.” As a result, “the government has no AIDS-awareness program of its own and restricts the public campaigns of independent family-planning groups.” [37] But, the article reported, “public health officials say they are stumped by a paradox in the Philippines, where a very low rate of condom use [4 percent] and a very low rate of HIV infection seem to be going hand in hand.”
In this conservative Catholic country that shuns condoms, about twelve thousand of the eighty-four million residents are infected with HIV. Jean-Marc Olive of the World Health Organization said that he’s not sure why this is, but he thinks they’re “lucky.” One gets the impression that “experts” would rather look puzzled than be forced to give credit to a chaste culture.
To appreciate the wisdom of the Filipino approach to halting the spread of HIV, contrast their efforts with the “safe sex” program implemented in Thailand. Both countries reported their first case of HIV in 1984. By 1987 there were 135 cases in the Philippines, and 112 in Thailand. The World Health Organization predicted that by 1999, 85,000 people would die of AIDS in the Philippines, and 70,000 in Thailand. In an effort to prevent this tragedy, Thailand enacted a “one hundred percent condom use program” and promoted widespread availability of condoms.[38] Meanwhile, the Filipino government backed the Church’s plan to prevent the epidemic.
By 2005, Thailand’s HIV rate was fifty times as high as the Philippines (580,000 vs. 12,000).[39] But because Thailand’s rate of new HIV infections is not as high as it used to be, it is hailed by “safe sex” experts as the model of how to protect a country against HIV. Health officials warn that an HIV epidemic has “the potential to explode” in the Philippines, but they are slow to acknowledge that if Filipinos hold fast to their morals, they’ll have nothing to fear.[40] Compared to Western culture, Filipinos have a delayed sexual debut and a reduced number of partners.[41] They are living proof that self-control always trumps birth control.
While some people see the Catholic Church as an obstacle to HIV prevention, the British Medical Journal noted, “The greater the percentage of Catholics in any country, the lower the level of HIV. If the Catholic Church is promoting a message about HIV in those countries, it seems to be working. On the basis of data from the World Health Organization, in Swaziland, where 42.6 percent have HIV, only 5 percent of the population is Catholic. In Botswana, where 37 percent of the adult population is HIV infected, only 4 percent of the population is Catholic. In South Africa, 22 percent of the population is HIV infected, and only 6 percent is Catholic. In Uganda, with 43 percent of the population Catholic, the proportion of HIV infected adults is 4 percent.”[42] In the Philippines, over 80 percent of the population is Catholic, and only .03 percent of the population has HIV![43]
The Catholic Church, like any good mother, wants what is best for her children. If your son or daughter had the chance to be sexually active with a person infected with HIV, what message would you give him or her? Would you entrust your child’s life to a piece of latex? Would you buy him or her a package of condoms, and then attempt to deliver a convincing abstinence message? Odds are, every loving parent would deliver an uncompromised message about abstinence. Why then would the Church do any less for her children?
Some argue that the Church’s opposition to condoms isn’t realistic because “some people are going to do it anyway.” But who are these “some people” who are incapable of being reached with the message of self-control? When I played college baseball, we were expected not to use steroids. Sure, some athletes do it anyway, but no coach would walk into the locker room and say, “We want you all to abstain from using performance-enhancing drugs. But since we know some of you will do it anyway, we’ll have a basket of free, clean syringes in the dugout.” Odds are, his players would not be inspired by his lack of confidence in them. If the coach truly cared about his players and wanted only the best for them, he’d motivate and empower them to make the best choice. In the same way, the Church will not give up on any human being but will continue to deliver the safest and healthiest message: chastity.
All of these considerations should offer more than enough evidence that the Church’s stance on contraception does not stem from naïve traditionalism. It comes, in the words of one Vatican reporter, “from a profound analysis of the need to integrate sexuality in an exclusive and permanent relationship open to life in the context of marriage. The wisdom of this view is becoming increasingly clearer.”[44] Critics may belittle the Catholic Church now, but as the saying goes, “All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self evident.”[45]
For more information on AIDS and Africa, visit our the “Research” tab above.
To study the success of abstinence education and the failure of “safe sex” promotion in Africa, you may wish to read Evidence that Demands Action by the Medical Institute for Sexual Health, or Rethinking AIDS Prevention by Edward Green, a Harvard senior research scientist.
_______________________________
[1]. Sue Ellin Browder, “Dirty Little Secret: Why Condoms Will Never Stop AIDS in Africa,” Crisis (June 1, 2006).
[2]. Tim Allen and Suzette Heald, “HIV/AIDS Policy in Africa: What Has Worked in Uganda and What Has Failed in Botswana?,” Journal of International Development 16:8 (November 8, 2004), 1141–1154; Michael Cassell, et al., “Risk Compensation: The Achilles’ Heel of Innovations in HIV Prevention?” British Medical Journal 332 (March 11, 2006), 605–607.
[3]. Craig Timberg, “Speeding HIV’s Deadly Spread,” Washington Post Foreign Service (March 2, 2007), A01.
[4]. N. Hearst and S. Chen, “Condom Promotion for AIDS Prevention in the Developing World: Is It Working?” Studies in Family Planning 35:1 (March 2004), 39–47, emphasis added.
[5]. Allen and Heald, 1141.
[6]. Edward Green, et al., Evidence That Demands Action (Austin, Tex.: Medical Institute for Sexual Health, 2005), ii.
[7]. Yoweri Museveni, 11th International Conference of People Living with HIV, as reported by Panafrican News Agency Daily Newswire (October 29, 2003).
[8]. Joseph Loconte, “The White House Initiative to Combat AIDS: Learning from Uganda,” The Heritage Foundation: Backgrounder 1692 (September 29, 2003).
[9]. Allen and Heald, 1141, emphasis added.
[10]. Arthur Allen, “Sex Change: Uganda v. Condoms,” The New Republic (May 27, 2002).
[11]. Allen and Heald, 1149.
[12]. D. Low-Beer and R. Stoneburner, “Behavior and Communication Change in Reducing HIV: Is Uganda Unique?” African Journal of AIDS Research 2 (2004), 2.
[13]. Edward Green, “Testimony before the Subcommittee on African Affairs,” Committee on Foreign Relations, U.S. Senate (May 19, 2003) 2.
[14]. Edward Green, “The New AIDS Fight: A Plan as Simple as ABC,” The New York Times (March 1, 2003).
[15]. Edward C. Green and Wilfred May, “Let Africans Decide How to Fight AIDS,” The Washington Post (November 29, 2003), A23.
[16]. S. Gregson, et al., “HIV Decline Associated with Behavior Change in Eastern Zimbabwe,” Science 311:5761 (February 3, 2006), 620–621; Richard Hayes and Helen Weiss, “Understanding HIV Epidemic Trends in Africa,” Science 311:5761 (February 3, 2006), 620–621.
[17]. Testimony of Edward C. Green, Ph.D., before the Committee on Energy and Commerce, U.S. House of Representatives (March 20, 2003), 3.
[18]. Green and May, A23.
[19]. Allen.
[20]. Rand Stoneburner, quoted in Allen.
[21]. Low-Beer R. Stoneburner, 1.
[22]. AnnaWald et al., “Effect of Condoms on Reducing the Transmission of Herpes Simplex Virus Type 2 from Men to Women,” Journal of the American Medical Association285 (June 27, 2001), 3103.
[23]. J. Thomas Fitch, “Are Condoms Effective in Reducing the Risk of Sexually Transmitted Disease?” The Annals of Pharmacotherapy 35:9 (September 2001), 1137; A. Saracco, et al., “Man-to-Woman Sexual Transmission of HIV: Longitudinal Study of 343 Steady Partners of Infected Men,” Journal of Acquired Immune Deficiency Syndromes6:5 (May 1993), 497–502; I. de Vincenzi, “A Longitudinal Study of Human Immunodeficiency Virus Transmission by Heterosexual Partners,” The New England Journal of Medicine 3331 (August 11, 1994), 341–346, as quoted in Fitch.
[24]. S. Ahmed, et al., “HIV Incidence and Sexually Transmitted Disease Prevalence Associated with Condom Use: A Population Study in Rakai, Uganda,” AIDS 15:16 (November 9, 2001), 2171–2179.
[25]. “New Research Confirms Condoms Not Effective in HIV Prevention,” LifeSiteNews.com (January 14, 2004).
[26]. Joshua Mann, et al., “The Role of Disease-Specific Infectivity and Number Of Disease Exposures on Long-Term Effectiveness of the Latex Condom,” Sexually Transmitted Diseases 29:6 (June 2002), 344–349.
[27]. R. E. Bunnell, et al., “High Prevalence and Incidence of Sexually Transmitted Diseases in Urban Adolescent Females Despite Moderate Risk Behaviors,” Journal of Infectious Diseases 180:65 (November 1999), 1624–1631.
[28]. Fitch, 1137.
[29]. “New Research Shows Dangers of Condoms in HIV Prevention,” Culture & Cosmos 1:23 (January 13, 2004), emphasis added.
[30]. D.T. Fleming and J.N. Wasserheit, “From Epidemiological Synergy to Public Health Policy and Practice: The Contribution of Other Sexually Transmitted Diseases to Sexual Transmission of HIV Infection,” Sexually Transmitted Infections 75 (1999), 3–17.
[31]. Peter Greenhead, et al., “Parameters of Human Immunodeficiency Virus Infection of Human Cervical Tissue and Inhibition by Vaginal Virucides,” Journal of Virology74:12 (June 2000), 5577–5586.
[32]. Nancy Padian, et al., “Heterosexual Transmission of Human Immunodeficiency Virus (HIV) in Northern California: Results from a Ten-Year Study,” American Journal of Epidemiology 146:4 (August 15, 1997), 350–357.
[33]. Dr. Daniel Low-Beer, as quoted by Alisa Colquhoun, “Ugandan Lessons?” Public Health News, February 6, 2004.
[34]. Fitch, 1137; Ronald Gray, et al., “Probability of HIV-1 Transmission Per Coital Act in Monogamous, Heterosexual, HIV-1 Discordant Couples in Rakai, Uganda,” Lancet357 (2001), 1149–1153; I. de Vincenzi, “A Longitudinal Study of Human Immunodeficiency, 341–346; Medical Institute for Sexual Health, Sex, Condoms, and STDs: What We Now Know (Austin, Tex.: Medical Institute for Sexual Health, 2002), 13.
[35]. Bluma Brenner, et al., “High Rates of Forward Transmission Events After Acute/Early HIV-1 Infection,” The Journal of Infectious Diseases 195 (April 1, 2007), 951–959; M. J. Wawer, et al., “Rates of HIV-1 Transmission Per Coital Act, by Stage of HIV-1 Infection, in Rakai, Uganda,” The Journal of Infectious Diseases 191:9 (May 1, 2005), 1403–1409.
[36]. Harvey Elder, “Human Immunodeficiency Virus (HIV),” a presentation at Health on the Horizon, sponsored by The Medical Institute for Sexual Health (June 13, 2002).
[37]. Seth Mydans, “Low Rate Of AIDS Virus In Philippines Is a Puzzle,” The New York Times (April 20, 2003).
[38], Human Life International, “Condom Exposé” www.hli.org, 16.
[39]. UNAIDS “Report on the Global AIDS Epidemic,” 2006, Annex 2, 511, 514.
[40]. Mydans.
[41]. Cecile Balgos, “Philippines Proud of its Low Infection Rate, Number of Cases,” San Francisco Chronicle (May 21, 2003).
[42]. Amin Abboud, “Searching for Papal Scapegoats Is Pointless,” British Medical Journal 331 (July 30, 2005), 294.
[43]. Bureau of Democracy, Human Rights, and Labor, “International Religious Freedom Report 2004,” U.S. Department of State (September 15, 2004); UNAIDS “Philippines” Country Situation Analysis (www.unaids.org).
[44]. “Doubts About Condoms: Science Questioning Their Efficacy in Halting HIV/AIDS,” Zenit Daily Dispatch, Nairobi, Kenya (June 26, 2004).
[45]. Commonly attributed to Arthur Schopenhauer.
You could respond in any number of ways. For one, you could ask the person, “If I can prove that the majority of high school students are virgins, will you be abstinent?” The most authoritative research on the sexual activity rates of high school students is the Youth Risk Behavior Survey conducted by the Centers for Disease Control. According to this nationwide survey of more than 150 high schools, only about a third of all students are currently sexually active.[1] Since 1991 teen sexual activity rates have been dropping, and now the majority of high school students are virgins.[2]
In fact, between 1991 and 2005 the sexual activity rate of high school boys dropped twice as quickly as that of high school girls![3] Among teens who have already lost their virginity, two-thirds of them wish they had waited longer to have sex (77 percent of girls and 60 percent of guys).[4]
The trend toward chastity is well underway, even if you haven’t noticed it on your campus. The National Campaign to Prevent Teen Pregnancy surveyed teens from around the country, asking them if it was embarrassing for teens to admit that they are virgins. Surprisingly, 87 percent of teens said no, it’s not embarrassing.[5] Most of those who said it was embarrassing were under the age of fifteen. Only 5 percent of older teens (fifteen to seventeen years of age) thought virginity was an embarrassing admission.
Despite the fact that these teens said virginity wasn’t something to be ashamed of, you don’t hear much about it because the sexually active students do all the talking. For some reason chastity gossip just doesn’t seem to spread as quickly. This gives the impression that “everyone is doing it,” when in reality the majority are not.
You could also point out that the “everyone” who is “doing it” is also getting STDs, that “everyone” is breaking up three weeks after they have sex, and “everyone” ends up getting divorced if they stay together long enough to get married. You are in no rush to join any of these crowds. We all have a fear of not being accepted or of being a loner if we do not conform to the world. But you must hold out for the higher standard of love.
The bottom line is this: What is your motivation? Is it to please God or to conform to the world and make life-changing decisions based on the opinions of classmates, most of whom you will probably never see again after graduation? Stay strong. You are worth the wait. Besides, the world needs to see young people who are not scared out of their minds to be chaste. This is something to be proud of, and if enough people on your campus realize this and have the courage to stand up, I would bet the saying “everyone is doing it” may eventually refer to chastity.
_________________
[1]. Centers for Disease Control, “Youth Risk Behavior Surveillance—United States, 2013.”
[2]. Centers for Disease Control, “Trends in the Prevalence of Sexual Behaviors: National YRBS: 1991–2007,” Fact Sheet (2008).
[3]. Centers for Disease Control, “Trends in HIV-Related Behaviors Among High School Students—United States 1991–2005,” Morbidity and Mortality Weekly 55:31 (August 11, 2006), 851–854.
[4]. National Campaign to Prevent Teen Pregnancy, “America’s Adults and Teens Sound Off About Teen Pregnancy: An Annual National Survey,” (December 16, 2003), 17.
[5]. The National Campaign to Prevent Teen Pregnancy, “The Cautious Generation? Teens Tell us About Sex, Virginity, and ‘The Talk,”’ (April 27, 2000), 1.
Some people think that chastity and virginity are synonymous, but they are not. Not all chaste people are virgins, and not all virgins are chaste. For example, before their conversions, Saint Augustine fathered a child out of marriage, Saint Margaret of Cortona lived with her boyfriend, and Saint Pelagia was a prostitute. While they may not have been virgins, they became chaste—and became saints.
On the other hand, some people are technically virgins, but they compromise their purity in countless ways. Many virgins assume, ‘‘As long as I retain my virginity, I’m being good. Therefore, everything short of intercourse is OK.’’ They may give parts of themselves to people they know they will never marry and assume that they are still pure because they are not having intercourse. Slowly they begin to believe that sexual intimacy is not a big deal. By the time they meet the person they truly deserve, they need a lot of healing for all they have given away.
But chastity is not something that can be lost forever because something shameful happened in your past. Virginity concerns our sexual history, but chastity is not concerned with the past. Chastity is a virtue that exists only in the present. People often think that because they have lost their virginity, purity will always be out of their reach. It is not. Just as a person who has led a pure life can fall into immorality, a person who has sinned can return to purity. To be pure it is necessary that your heart be directed to God. In his eyes, the repentant prostitute is purer than the lustful virgin. We need to remember that our worth lies in how God sees us, not in how others see us or even in how we sometimes see ourselves.
Look at both these issues and judge for yourself if contraception is part of the solution or part of the problem.
Because of the widespread use of birth control, more people than ever have sex without intending to have children. Sex out of wedlock has become far more common, and more sex means more babies. Some argue that teaching people how to use contraceptives will alleviate the problem. But research shows that “programs in safer sex education and condom distribution have not reduced the out-of-wedlock birth rates among sexually experienced teens. . . . The fact is, increased condom use by teens is associated with increased out-of-wedlock birth rates.”[1]
In Colorado, one school began passing out condoms to the students. Within three years the birth rate rose 31 percent above the national average, and in one school year one hundred births were expected among the twelve hundred students. The administrators were described as “searching for explanations.”[2]
When unwanted pregnancies occur, many turn to abortion as a solution. In fact, studies show that about half of all unintended pregnancies end in abortion.[3] Some argue that increased use of contraception could have lowered these abortion rates. However, the research institute of the nation’s largest abortion provider admits that most women who receive abortions had been using birth control during the month they became pregnant![4]
Such couples feel that the “fault” of the pregnancy can be blamed on the failed contraception, but by contracepting they have already set their wills against new life. Since contraception treats pregnancy as if it were a disease, many people conclude that abortion must be the cure. I once saw a condom advertisement that called pregnancy “the mother of all nightmares.” With this mentality it is no surprise that the sex researcher Alfred Kinsey said, “At the risk of being repetitious, I would remind the group that we have found the highest frequency of induced abortion in the group which, in general, most frequently used contraceptives.”[5] Even a former medical director of Planned Parenthood admitted in 1973, “As people turn to contraception, there will be a rise, not a fall, in the abortion rate.”[6] Fifty million abortions later, no one can dispute his prediction.
Lastly, it should be noted that anyone who believes that contraception decreases abortions ignores the fact that hormonal birth control can cause abortions.[7] Click here for details on that.
Mother Teresa did not need to see the statistics. She was well aware of the connection between contraception and abortion when she said in a speech in the presence of Bill and Hillary Clinton:
“The way to plan the family is Natural Family Planning, not contraception. In destroying the power of giving life, through contraception, a husband or wife is doing something to self. This turns the attention to self and so destroys the gift of love in him or her. In loving, the husband and wife must turn the attention to each other. Once that living love is destroyed by contraception, abortion follows very easily.”[8]
__________________
[1]. The Consortium of State Physicians Resource Councils, “New Study Shows Higher Unwed Birthrates Among Sexually Experienced Teens Despite Increased Condom Use” (February 10, 1999).
[2]. Jana Mazanee, “Birth Rate Soars at Colorado School,” USA Today, May 19, 1992, 3A.
[3]. Stanley Henshaw, “Unintended Pregnancy in the United States,” Family Planning Perspectives 30:1 (1998), 24–29, 46.
[4]. Rachel Jones, “Reported contraceptive use in the month of becoming pregnant among U.S. abortion patients in 2000 and 2014,” Contraception 97 (2018) 309–312; Rachel Jones, et al., “Contraceptive Use Among U.S. Women Having Abortions in 2000–2001,” Perspectives on Sexual and Reproductive Health 34:6 (November/December 2002), 296.
[5]. Mary S. Calderone, ed., Abortion in the United States: A Conference Sponsored by the Planned Parenthood Federation of America and the New York Academy of Medicine (New York: Harper and Row, 1958), 157.
[6]. Malcolm Potts, Cambridge Evening News, February 7, 1973, as quoted in “The Connection: Abortion, Permissive Sex Instruction, and Family Planning,” Life Research Institute (January 2000).
[7]. Walter L. Larimore and Joseph B. Stanford, “Postfertilization Effects of Oral Contraceptives and Their Relationship to Informed Consent,” Archives of Family Medicine 9 (February 2000), 126–133.
[8]. Mother Teresa, February 5, 1994, National Prayer Breakfast, Washington, D.C.
In 2000 the National Institutes for Health (NIH) published the first thorough review of the scientific research on condom effectiveness.[1] The study examined eight STDs and demonstrated that condoms reduce the risk of contracting or transmitting two of them: HIV and gonorrhea (in men). The studies revealed that, when consistently and correctly used, condoms provide an 85 percent risk reduction for the transmission of HIV in males and females and a 45 to 75 percent risk reduction for the transmission of gonorrhea in males.
While the condom may reduce the likelihood of contracting HIV, yearly cases of this virus are much less than 1 percent of all the yearly STD cases.[2] Gonorrhea is a much more common problem, but there was not sufficient evidence to determine how much protection condom use offered women. This is not good news for women, because they suffer much greater consequences from being infected by this disease. It can lead to ectopic pregnancy, pelvic inflammatory disease, and infertility. In regard to the other specific diseases, the report stated that “there was no evidence that condom use reduced the risk of HPV infection.”[3]
Furthermore, the data were unable to determine how effective the condom is in reducing the risk of the other STDs. In spite of all the talk today about condoms and safe sex, they could not say what degree of protection condoms offered for most of the STDs reviewed! This is troubling, considering that these diseases infect millions of people each year and can make them at least two to five times as likely to transmit HIV.[4]
While the NIH study does not prove that the condom is useless in protecting against the STDs mentioned above, it does mean that twenty-eight expert panel members scouring through 138 peer reviewed studies on condom effectiveness were unable to determine its effectiveness. Since the publication of this study, others have determined that the condom use reduces STD risks only by about half.[5]
In the wake of the NIH report, politicians who favor promotion of “safe” sex were livid, arguing that the publication of such information could contribute to a rise in STDs because it undermines public confidence in the condom.[6] What they didn’t want to admit was that the outdated message of “safe sex” causes people to be overconfident in the condom. One scientist noted:
“Some fear that informing the public of how little we know about condom effectiveness would lead to nonuse of condoms. Although it is improbable that any scientific evidence supports this hypothesis, the question remains. Is it ethical for health care professionals, including physicians and pharmacists, to hide the truth from the public? As in every other area of health care, we must give accurate data as we attempt to steer our patients toward the healthiest and safest choices. Ultimately, each individual must decide how much risk he or she is willing to take. But such a decision can be made responsibly only if individuals are accurately informed about the degree of risk they face (or may face) if they choose to be sexually active.”[7]
Determining the effectiveness of condoms in preventing STDs is a complicated matter. For example, some STDs, such as chancroid or gonorrhea, transmit very easily, while others, such as HIV, are not as contagious. Some STDs, such as herpes, change their infectivity over time. One week the person could be shedding the virus, and a week later, not shedding. Factors such as gender, stress, drug interactions, pregnancy, and the presence of another STD also play a role in STD transmission. In fact, each person’s immune system is unique in how well it resists infections. For all of these reasons and more, it is difficult to pinpoint a precise level of condom effectiveness for STDs in general.
When determining the effectiveness of the condom in preventing the spread of STDs, it’s enlightening to examine how well the condom prevents pregnancy. According to the research institute of Planned Parenthood, the failure rate of the condom in preventing pregnancy is 15 percent during the first year of use.[8] Considering that a woman can get pregnant only a few days of the month and STDs can be contracted any day, the condom is by no means adequate protection. No matter what STD we are speaking about, the condom does not guarantee protection even when used consistently and correctly. On the other hand, chastity guarantees 100 percent protection.
But the bottom line is this: There is no condom for the heart or the soul. Whatever we may do to protect our bodies from STDs, if we misuse God’s gift of sexuality, our hearts and souls will not escape the consequences. But if we are faithful with our sexuality, there is no need for protection of any kind, for there is nothing to fear. The very idea of wanting to make sex “safe” is a contradiction in terms. Sex is meant to be a total gift of the self, holding nothing back. Concerns about “safety” should not enter into the equation. You protect yourself from your enemies; you give yourself to your beloved.
_______________________________
[1]. National Institutes of Health, “Scientific Evidence on Condom Effectiveness for Sexually Transmitted Disease (STD) Prevention” (June 2000).
[2]. John Diggs, M.D., “NIH[National Institutes of Health] Report Collapses Foundation of Comprehensive Sex Education,” Abstinence Clearinghouse, August 6, 2001.
[3]. NIH, “Scientific Evidence on Condom Effectiveness for Sexually Transmitted Disease (STD) Prevention,” 26.
[4]. U.S. Department of Health and Human Services. “Scientific Review Panel Confirms Condoms Are Effective Against HIV/AIDS, But Epidemiological Studies Are Insufficient for Other STDs,” by HHS News, press release, July 20, 2001.
[5]. L. Manhart, L. Koutsky, “Do Condoms Prevent Genital HPV Infection, External Genital Warts, or Cervical Neoplasia? A Meta-Analysis,” Sexually Transmitted Diseases29:11 (2002), 725–735; S. Vaccarella, et al., “Sexual Behavior, Condom Use, and Human Papillomavirus: Pooled Analysis of the IARC Human Papillomavirus Prevalence Surveys,” Cancer Epidemiology Biomarkers & Prevention 15:2 (2006), 326–333; R.Winer, et al., “Condom Use and the Risk of Genital Human Papillomavirus Infection in Young Women,” The New England Journal of Medicine 354:25 (2006), 2645–2654; S. Ahmed S, et al., “HIV Incidence and Sexually Transmitted Disease Prevalence Associated with Condom Use: A Population Study in Rakai, Uganda,” AIDS 15:16 (2001), 2171–2179; J. Baeten, et al., “Hormonal Contraception and Risk of Sexually Transmitted Disease Acquisition: Results from a Prospective Study,” American Journal of Obstetrics & Gynecology 185:2 (2001), 380–385; J. Shlay, et al., “Comparison of Sexually Transmitted Disease Prevalence by Reported Level of Condom Use Among Patients Attending an Urban Sexually Transmitted Disease Clinic,” Sexually Transmitted Diseases 31:3 (2004), 154–160; A. Wald, et al., “Effect of Condoms on Reducing the Transmission of Herpes Simplex Virus Type 2 from Men to Women,” Journal of the American Medical Association 285:24 (2001), 3100–3106.
[6]. Nancy Pelosi et al., “Pelosi and House Colleagues Criticize Administration Report for Undermining Condom Effectiveness: Members Request Study Guided by Science Not Ideology,” press release, Washington, D.C. (July 24, 2001) as referenced in note 10, “The NIH Condom Report: The Glass is 90% Full,” by Willard Cates, Jr., Family Planning Perspectives 33:5 (September/October 2001), 232.
[7]. J. Thomas Fitch, “Are Condoms Effective in Reducing the Risk of Sexually Transmitted Disease?” The Annals of Pharmacotherapy 35:9 (September 2001), 1137.
[8]. Haishan Fu, et al., “Contraceptive Failure Rates: New Estimates From the 1995 National Survey of Family Growth,” Family Planning Perspectives 31:2 (March/April 1999), 60.
I would recommend three things. First, pray and fast for your school. In the Gospel of Mark, Jesus spoke about how some people could only be healed of their spiritual illness through other people’s prayer and fasting for them (9:29).
Second, one of the most effective things you can do to spread the message of chastity is to live it. This is because the virtue of purity is more easily caught than taught. As Saint Francis said, ‘‘Preach the gospel always. When necessary, use words.’’ Your silent example comes first. If you are in a dating relationship, make sure that God is the center of it so that your classmates will see what joy a godly relationship can bring. Even if you are not dating anyone, your witness of purity is just as powerful. To quote Saint Paul, ‘‘Let no one despise your youth, but set the believers an example in speech and conduct, in love, in faith, in purity’’ (1 Tim. 4:12).
The world seriously doubts that chastity can exist in the lives and relationships of modern couples. It refuses to believe that two young people madly in love with one another can resist temptation. What the world does not see is that as long as the couple have a motive—true love—it is very possible. Not only is it possible, but Mary Beth Bonacci observed that couples who live chastity ‘‘were having an easier time getting out of bad relationships. They were making better marriage decisions. They were happier.’’[1] Therefore, be a light to the world. Your school needs to see that we do not embrace chastity because we’re afraid of venereal infections or unwanted pregnancy.
Everyone is aware of the sexual messages that bombard us on every television channel and radio station. The message of ‘‘sexual liberation’’ surrounds us. Unfortunately, to curb this permissiveness, the message of purity has often been couched in terms like ‘‘Just say no,’’ ‘‘True love waits,’’ ‘‘Abstain.’’ All of these slogans are good, but they can create the impression that purity is nothing more than a system of restraints. This may not appeal to a person who only knows the immediate ‘‘love’’ and affection of purely physical relationships. Because of this, the message of chastity needs to be rehabilitated so that everyone will be able to see the clear and obvious link between true love, total freedom, and purity. It is not about avoiding STDs. It is about having a better kind of love. Most importantly, it is about wanting heaven for the person you love.
Third, to get this message out, I would recommend starting a chastity club at your high school or college. This is not an abstinence bereavement group but an apostolate to spread the message of chastity courageously. Through the club, you can connect with students who share your passion for purity and launch any number of projects and activities to transform your campus. Some of the projects involve visiting local high schools or junior highs to spread the message of chastity to younger students. Considering that there are over sixteen million high school students in America, there is much work to be done.[2] If your school is Catholic, another goal of the club can be to start up Eucharistic Adoration on your campus, with the help of the chaplain or campus minister. This has an unspeakable power to sanctify the students (and faculty) because you are bringing Christ Himself into their midst. In the words of Pope John Paul II,
“The Eucharist is the secret of my day. It gives strength and meaning to all my activities of service to the Church and to the whole world. . . . Let Jesus in the Blessed Sacrament speak to your hearts. It is He who is the true answer of life that you seek. He stays here with us: He is God with us. Seek Him without tiring, welcome Him without reserve, love Him without interruption: today, tomorrow, forever.”[3]
One girl said after hearing a talk on sexual purity, ‘‘I agree with everything you say. I know most of my friends would, too. It all makes so much sense. It’s just that no one else I know is actually doing it. I don’t know if I’m strong enough to be the first one. Maybe if a group of us all started together.’’[4] This is your job—to create a culture in which it is easy to be good, a climate favorable to purity. In the words of Saint Catherine of Siena, ‘‘If you are what you should be, you will set the world on fire.’’[5]
______________________________
[1]. Mary Beth Bonacci, ‘‘Expressing Love: How to Speak the Language of Permanence,’’ Be, May–June 2000, 10.
[2]. ‘‘Digest of Education Statistics Tables and Figures, 2005,’’ The National Center for Education Statistics, U.S. Department of Education.
[3]. Pope John Paul II, L’Osservatore Romano 41 (October 8, 1997), 7.
[4]. Shalit, A Return to Modesty, 229.
[5]. St. Catherine of Siena, letter 368.
When I played college baseball, we were expected not to use steroids. Sure, some athletes do it anyway, but no coach would ever walk into the locker room and say, “We want you all to abstain from using performance enhancing drugs. But since we know some of you will do it anyway, we’ll have a basket of free, clean syringes in the dugout,” with a special class for those who don’t want to abstain.
The same goes with the condom. If you had a child who was thinking about sleeping with a person who might have HIV, would you say, “I’d rather you not sleep with that person. But, since I know you’ll probably do it anyway, here’s a condom?” There’s no way you would entrust the life of your child to a thin piece of latex. You would give him or her a clear and uncompromised message of purity. Doesn’t every person deserve to hear the same message you would deliver to a person you love? Every human being is capable of self-control, and is able to make smart decisions. If anything, the people who are “going to do it anyway” are the ones most in need of a convincing abstinence message.
Besides, what if you taught students how to use a condom, and then a young woman returned to you two years later, asking how she got cervical cancer, despite using a condom every time? What would you tell her?
The fact is that most people who promote the outdated and medically inaccurate notion of “safe sex” are unaware of the condom’s failure rate in preventing STDs. Most people also underestimate the failure rate of contraception in preventing pregnancy, falsely assuming it’s 99% effective. A former medical director for Planned Parenthood once wrote, “More than three million unplanned pregnancies occur each year to American women; two-thirds of these are due to contraceptive failure.”[1]
The notion of “safe” sex is misleading because it gives people a false sense of security to engage in risky behavior. For example, when a teenage girl becomes sexually active, she becomes more likely to become depressed, have more breakups, and eventually get divorced, as can be seen in this study of 10,000 women. Other studies also show that sexually active girls are more likely to attempt suicide. Obviously these things don’t happen to every sexually active teen, but the sooner a woman becomes sexually active, the more likely she is to suffer through them. With that in mind, it seems pretty misleading to call sex “safe” because a piece of latex is involved. Promoting safe sex makes as much sense as telling your child to wear a helmet if he’s going to play in traffic.
Lastly, the whole idea that teens are “going to do it anyway” is equivalent to saying that you’re giving up on them. After my wife and I gave a chastity talk at a school, a girl from the audience came up to Crystalina and dropped something in her hand, saying, “Thanks for the talk. I won’t be needing these anymore.” My wife looked down, and in her hand was a half empty packet of birth control pills. Now, do you think this girl would have been that impacted by our talk if we concluded it by passing out condoms for those who were “Gonna do it anyway”?
It is impossible to deliver a convincing abstinence message while promoting condoms, as can by seen by how ineffective “comprehensive” sex-ed has been. Abstinence educators are not naive about the sexual activity levels of teens. They’re just the ones who know what’s at stake. For proof that abstinence education works, click here.
___________________________
[1]. Dr. Louise Tyrer, Letter to the Editor, Wall Street Journal, 26 April 1991.

